一人一個移民的故事 英國心泉除了在大倫敦區舉辦支援移英青少年的表達藝術治療小組外,THRIVE LDN 也資助我們為年青人的家長提供敘事實踐(Narrative Practice)小組。

你的自我感覺會大大影響你與他人的溝通和聯繫方式。如果你認為自己很沉悶、很奇怪或者很麻煩,你可能會不太願意伸出援手。害羞和社交焦慮會導致孤立感,那會加劇你的不安全感。以下幾點要謹記:

孩子出現情緒困擾,適當的輔導和治療能夠幫助他們走出困境。英國心泉提供的服務分為兩類:(一)由本會的專業人士提供免費或資助之輔導或治療服務;(二)轉介其他專業人士和機構。

當廿多歲自閉症譜系的仔仔想發脾氣時就和他行斜路及雙手放頭上再用力壓頭頂,這個多星期來都能有效協助仔仔舒緩情緒。

兒童及青少年出現情緒及精神健康問題時,英國國民保健服務(NHS)提供的支援,分為四級。

建議青少年在上學日晚上至少睡8至10個小時。以下方法可確保你的孩子有足夠的睡眠,以保持健康,並在上學前得到充分的休息

在英國,為有精神健康需要,或有特殊教育需要和殘疾的兒童和青少年(SEND)尋找支援服務,家長可以有以下的途徑
一個十來歲的小孩,放學後揹着書包,連校服都未換,便匆匆登上了巴士,直往他的目的地 — 機場。要搭飛機嗎?一個人要去哪兒呢?他的口袋裡明明没有錢買機票啊。

安娜.弗洛伊德中心 (Anna Freud Centre) 的臨床醫生研發出以下七種方法,相信是回應兒童和青少年的 擔憂的最佳做法。

當事情未如理想、遇上不公平的事或別人傷害我們時,憤怒是一種再正常和健康不過的反應。憤怒讓我們知道有問題或不妥。

要離開自己成長的香港移遷外地,對大部分家庭都是前所未有的經驗和挑戰,尤其
是孩子,他們大多是跟隨父母的決定,離開自己熟悉的環境。面對這些重大轉變,
無論什麼年紀的孩子也承受著很大壓力。

如果您認為您的孩子可能患有抑鬱症,讓他們儘早獲得幫助是一件很重要的事。拖延得越久,成為長期問題的風險就會更高,而且越有可能擾亂您孩子的生活。

我們是一群和你一樣移居英國的香港註冊社會工作者,加入了「英國心泉」成為義工負責家長支援的工作,希望能盡綿力陪伴移英的家長,大家一起探索協助子女適應英國生活的方法,讓家長與孩子並肩同行闖過難關。

兒童不時感到擔心或焦慮是正常的 - 例如當他們開始上學或上託兒所,或搬往新地方。但是對於一些孩子來說,焦慮每天都影響他們的行為和思想,干擾了他們在學校、家庭和社交生活。這種情況下,你或需專業人士幫手解決。
如果你有一些很可怕的經歷,例如暴力、侵犯、強姦或生命受到受威脅,就有可能出現創傷後遺症。如果你曾經目睹一些可怕的事情,例如嚴重意外,亦有可能有創傷。

當孩子因為面對挑戰和不明朗而感到擔憂時,要告訴他這是正常不過的。你可以傾聽孩子的擔憂,鼓勵他們發問,以肯定您是否真的理解孩子的想法,也可以嘗試用實際的資料或例子來回答他們的問題。
有些兒童和青少年喜歡上學,但另一些卻很掙扎—他們困在家裡,遠離朋友。有些可能正面對家庭問題,又或生活上出現種種缺失或變化,讓他們感到焦慮不安。

自殘是指某人以故意傷害自己,來應對痛苦或不堪重負的感受和經歷。自殘的人可能有很多強烈的想法和感受難以處理,因而覺得傷害自己是唯一的應對方法;他們也可能是感到麻木,因而以傷害自己來獲得某些感覺。

孩⼦和年輕⼈不時會擔⼼學校裏發⽣的事情,這是正常不過的。最重要是去
承認有問題需要解決,並且與年輕⼈及學校合作,盡快尋求合適的⽀援。

兒童有時其實只須要有人願意聽聽他們的心底話,但是情緒問題已開始對其生活做成影響,則須要尋求專業意見。

對於不少孩子而言,要講心事已經不容易,要用非母語講則更困難。我們的團隊希望扮演橋樑角色,以廣東話為學童提供精神健康評估,再撰寫英文轉介信,方便家長與本地醫護人員及老師跟進。

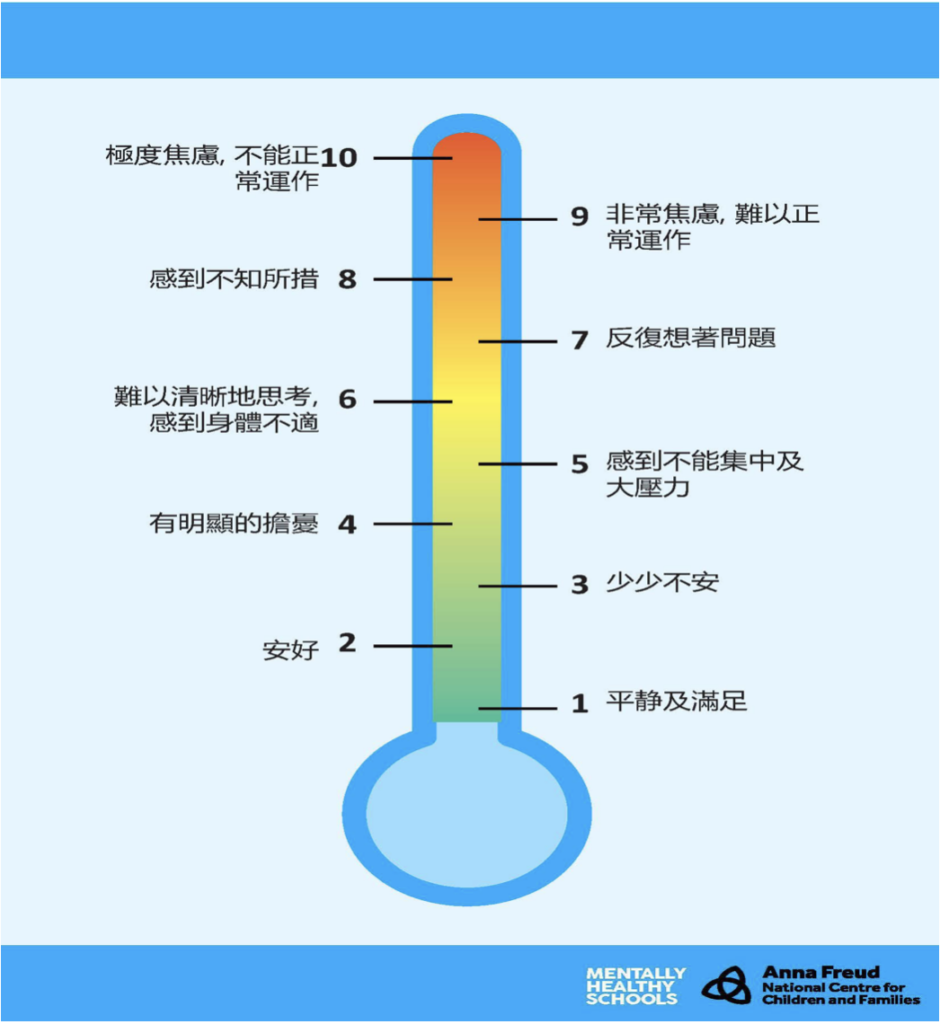
在這個盒⼦裡,你要放入令你安穩下來、感覺放鬆、減少恐慌、焦
慮或情緒的東西。

「教育、健康及照顧」(下稱EHC)計劃是一個專為25歲或以下,有需要更多特殊教育支援的兒童及青少年而設的。這個計劃會確認特殊教育需要(SEN)人士的教育、健康和社交需要,及針對他們所需而設定額外的支援和津助。

英國心泉成立而來,收到不少家長查詢,苦惱於如何為子女在英國尋求情緒支援服務。
同完GP講,GP叫搵學校,學校又叫搵返GP。究竟要搵邊個?
究竟CAMHS(兒童及青少年精神健康服務)要點先申請到?
點係居所附近幫仔仔女女搵輔導?
在香港已確診有自閉症或ADHD,來到英國是否要找CAMHS重新做評估?
你是否有上述的經歷?任職CAMHS的精神健康工作員HEI TING為你介紹NHS、學校及社區的兒童及青少年情緒支援服務。
https://ghc.nhs.uk/wp-content/uploads/CAMHS-Guidelines-for-Referers-with-LD-June-2015-Final.pdf
https://www.nottinghamshirehealthcare.nhs.uk/camhs-referral-criteria
https://secureforms.oxfordhealth.nhs.uk/camhs/professional.aspx
(Chinese version only)

Referrals can be made by a variety of agencies including:
理論上,上述渠道和人士都可以直接轉介兒童或青少年接受評估,以決定是否獲得CAMHS支援。但從我們所處理的個案所見,上述人士不少都會先轉介當事人給普通科醫生,由後者再做轉介。
若情況非常緊急,請致電111或查閱下列網站以找可提供的即時服務 https://www.nhs.uk/nhs-services/mental-health-services/where-to-get-urgent-help-for-mental-health/ 或當區的危機處理小組熱線 https://www.nhs.uk/service-search/mental-health/find-an-urgent-mental-health-helpline/location
GP即普通科醫生,他/她照顧你孩子身體和精神健康。你可致電附近診所,預約已登記的GP或其他GP 。
你的普通科醫生可提供以下協助:
GP一般會先接見你的孩子,才作轉介。如果你的孩子暫時不願意求診,你可以自己約見GP,講述有關情況,並要求獲取相關資料及建議。
診所一般有即日緊急預約服務;如果你孩子的情況緊急,請盡早致電診所。
求診前,你的孩子可以先閱讀《第一次見GP會做咩?》。
他們通常第一次會寫信與你聯絡,告訴你約見的日期。當你收信時,這可能只是邀請該有困難的孩子及你們 (身為父母親/照料者) 見面,或者可能會邀請全家人見面。你亦可能會接到電話問你是否已收到來信,及看看你們是否可以出席。
你可能在收信後要等數星期才到約見日期,因為很多 CAMHS 組都非常忙碌。如果 你在等候約見期間認為你孩子的問題愈來愈嚴重,請通知 CAMHS 組 – 他們也許 能提議在等候面談期間,你可以做些甚麼去幫助你的孩子。
CAMHS 組在很多不同的地方工作,包括他們自己的診療室,或會派工作人員到你 的家中、孩子的學校,或你醫生的診所與你們會面。大多數約見都是在星期一至五日間時間進行,但如可能的話,他們也許能安排在放學後或黃昏的時間。在首次會面時,你與孩子會與在 CAMHS 組工作的一位或兩位人士會面。視乎孩子的年齡,他們亦可能會要求單獨與你的孩子會面。
由於精神健康問題並不如身體健康問題那麼明顯,因此你應該:
工作人員希望能在這首次會面中,從你與孩子盡量得到更多資料,以便他們能與 你及孩子一起計劃你們可能需要甚麼協助。這時最重要的是要提出所有問題,及 確保你明白他們告訴你的事情。
第一次會面一般是一小時。
第一部份: CAMHS團隊成員會先了解孩子的家庭狀況,例如有沒有兄弟姐妹,從中繪製家庭關係圖,這有助 他們了解孩子苦惱之源,是否與家庭問題(例如父母離異)有關,並探討你和家人的關係; 他們也可能會詢問孩子的童年,這將有助他們分析你面臨的問題,是否存在已久。 這部分通常和你們一家在同一會見室內進行。
第二部份: 由孩子講講被轉介到CAMHS做評估的原因,團隊成員會詢如果孩子在這部份呢希望單獨傾,團隊會安排你們先離開。
第三部份:CAMHS人員會根據轉介人描述孩子的情況,向他/她了解多啲,具體問題會因應他/她面對的狀況和困難而異。
第四部份:父母會再度加入,一起討論用最好的方法協助孩子康復。
CAMHS 會決定他們的服務是否適合孩子,如果合適,就會加入CAMHS服務輪候名單。否則,他們會轉介孩子去更為合適的服務,例如一些非政治組織提供的支援。與你們傾談後,他們可能會建議:
輔導及治療(心理治療)以傾談為主,有時會加入藝術或其他創意元素,讓孩子表達和抒發感受丶思緒和經驗,從而了解生命中的經歷和找尋應對困難的方法。
你可透過以下途徑,為孩子安排輔導及治療:
英國不同組織有提供很多毋須轉介的服務,其中包括任何人都能致電的緊急求助熱線。
你可以查看一些為青年提供心理健康支援的本地服務,包括電話號碼和網站資料。(只有英文資料)
你可以查看屬義務性質、以社區為基礎的青少年資訊服務,它們大多提供諮詢和專業支援會面。(只有英文資料)

The follow is the approach of assessment and questions that are likely to appear in an assessment appointment. A good preparation and the provision of the right information will help in getting the appropriate supports for the children and young people.

Specialist CAMHS services are available to children and young people who have severe, complex and enduring emotional/behavioural/mental health difficulties. Specialist CAMHS services are, for example, not appropriate for children / young people who are experiencing a normal reaction to a significant life event (e.g. a normal bereavement or a normal reaction to parental separation). A good understanding of the service scope and assessment criteria will help clients in getting the right service.
This includes children and young people with specific as well as mild learning disabilities. The mental health needs of children and young people with more moderate to severe learning disability are provided for by specialist teams. There is a CAMHS Learning Disability Team and Child Disability Team in most of the areas.
The CAMHS team will allocate an assessment appointment based on need, judged by:
Specialist CAMHS will accept referrals of children and young people whose symptoms or distress and degree of social and/or functional impairment are severe. The emotional health and wellbeing difficulties need to have a noticeable and substantial impact on a number of areas of functioning: e.g. school, home and social situations.
Usually, the duration of these difficulties should be not less than three months. For severe / life-threatening conditions (see above) and for other conditions where there is severe impairment of functioning, the referral should be made immediately.
Where the child/young person’s symptoms persist beyond this time, and/or they are non-responsive to first line interventions (e.g. school support, community services), i.e. the difficulties are worsening/persisting despite front line interventions being in place e.g. ELSA in school, community parenting support, GP directed self help, they should be referred to CAMHS.
Evidence of recent typical external stressors e.g. family breakdown, bereavement, exams, hospital visits (past or impending) where sufficient time has been allowed for the child to adjust and/or recover with help from immediately available resources
A child/young person should be seen urgently if there is a reported sudden onset of symptoms, symptoms are causing substantial distress or there is probable risk of harm to self or others due to level of difficulty.
Specialist CAMHS will accept referrals where there is a likelihood that the child or young person has a severe mental health disorder.
Specialist CAMHS will accept referrals where there is a high level of case complexity. This might include, for example, multiple risk factors, complex family problems, child protection concerns, such as parental mental health, history of abuse, familyDisruption. Concerns of risk that is ongoing e.g. domestic abuse, physical chastisement, significant substance use, exploitation, risks posed by significant others.
In order to improve accessibility for children and young people, the team will find the following not appropriate for referral to specialist CAMHS:
These are sometimes called “normal adjustment reactions”. Unfortunately, we are unable to provide a service to children and young people whose difficulties are associated with a normal reaction to recent life events (e.g. bereavement, parental separation, physical illness). If intervention is required, these children and young people are usually best helped by counselling, and it is not necessarily appropriate to identify the child/young person with the specialist CAMHS service.
Please note that specialist CAMHS does not provide a service for children and young people whose problems are solely related to specific learning or behavioural difficulties within the classroom or other difficulties which occur only at school (e.g. behaviour settled at home; unsettled in school). For these children/young people it is usually more appropriate for educational services to become involved to address the difficulties.
Single symptom such as sleeping difficulties, minor eating problems, toileting issues would not meet CAMHS criteria and should be provided by universal or targeted services (e.g. primary care, local service teams) in the first instance.